

It’s 2017 and we are still having arguments about how Healthcare works (or doesn’t) in the United States. Yet somehow none of the pundits have a single well-informed thought to share. It’s like that Indian parable where blind men argue about an elephant.
Well, I am a bonified Healthcare IT Nerd who spent over a decade specializing in Revenue Cycle Management (RCM). I have met over a thousand physicians from the whole range of specialties and hundreds of their billing managers. My special lady is a physician who sees patients across the economic spectrum (we discussed billing codes on our first date, it was very romantic). And my friends and family have experienced the entire gamut of illness from pediatric cancer to MS to Alzheimer’s.
There are people who know much more about healthcare than I do, but in the pachyderm metaphor I qualify as a one-eyed man and I have four true things to tell you about American Healthcare.
I. We’re Very Bad At Estimating Personal Risk
In 2014, a wide swath of my friends and family became concerned about the rise of ISIS and its threat to our safety. A smaller, but no less earnest group of my friends was (and remains) concerned about random acts of violence, so they carry concealed weapons.
Respectfully, CDC mortality data from 2014 shows that both groups paid attention to the wrong things. Bees killed four times as many Americans in 2014 as terrorism. And as for homicide (both murder and manslaughter), it ranked a distant 17th:
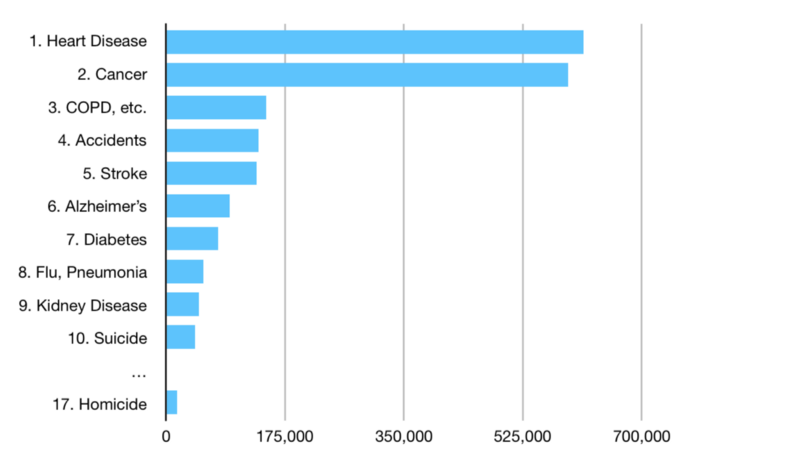
Suicide is three times more likely to kill you than any kind of homicide. According to the FBI, only 12% of homicides in 2014* were carried out by complete strangers. So you’re 430 times more likely to be killed by your diet than a random act of violence. You know what that means?
The assassin stalking you is Ronald McDonald.
Americans have no idea what their health risks are. That’s because we think in narrative instead of number. Terrorist attacks seem totally real because they do news stories about those. CNN doesn’t break in with a special report after you eat a Triple Baconator instead of a salad, but maybe they should.
“Sources on the scene initially believed the individual just wanted bacon but it has come to light that the Classic Cobb Salad also includes bacon. Authorities are now investigating the possibility that this man, James Michael Allen, was motivated by the Baconator’s triple cheese. If he continues his burger spree it will lead to obscene medical bills and a shortened lifespan. For special coverage on this developing story, we go now to Wolf Blitzer in the Situation Room,”
Don’t listen when people say they don’t need coverage because they’re too whatever (young/old, gay/straight) to get sick. And if they say that they don’t need health insurance because they’re just gonna ‘tough it out’…

Also my face when someone says ERs count as ‘universal coverage’
II. You Always Pay For Insurance You Can’t Use
Let’s say you drive a sweet diesel F-250 like this:

Super Duty, Son.
That’s a great truck. You have excellent taste, my friend. Best-in-class towing capacity. The legendary Powerstroke engine. I especially love the color.
Anyway, let’s say your car insurance is from Acme Mutual. They have such great service that your neighbor Ned switches his policy. A day later, he gets T-boned by an uninsured driver. Ned drives… this:

The 2014 Honda Fit EV does not have legendary towing capacity
The dollars you paid to protect your beautiful F-250 are now being used for repairs you’ll never need. There’s no special “Electric Vehicle Repair’ fund set aside for Ned’s car, it’s just Acme’s pool of reimbursement money.
In 2014, there were less than 14 claims paid for every 100 insured automobiles. Those claims constituted less than 25% of the premiums paid during that period. In other words, Ned’s EV-related repairs (whatever they are) contribute a tiny amount to your premiums.
A similar principle is true in healthcare**: According to the CDC, physician office visits are less than 20% of US healthcare spending. A fraction of that is age or gender-specific preventive care. The vast bulk of health spending goes to expensive hospital services. We spend most of our healthcare dollar on treating problems when they’ve gone too far to treat in a clinic.
Hospitalizations are the ‘multi-car pile-up’ of healthcare spending. Very sick people can cost $20,000+ per day to admit to a hospital. So the best way to control costs is to keep people healthy enough to avoid hospitalization. If you start carving off relatively tiny preventive costs (e.g., gynecological or prostate exams) because “not everyone needs it” you’ll end up causing more hospitalizations through neglect and premiums will rise.
Moreover, it’s really hard to know which cut will break the camel’s back without studying specific, local situations. I spoke with an ACO data scientist once who found that his organization could cut hospitalizations by 20% if they gave the sickest people a bus pass. The patients were so sick that they didn’t have reliable transportation to keep urgent appointments they needed when their symptoms flared. A bus pass was all it took to keep them well.
You wouldn’t demand that Acme sell you a policy where your premiums won’t be used to pay for Ned’s repairs. So don’t listen when someone demands a policy that only covers the kinds of problems they personally have. That’s not how insurance works.
III. We Already Have ‘Socialized Medicine’
According to the OECD, U.S. per-capita health expenditures were ~$9500 in 2015. Roughly half of that, ~$4750, was paid by some level of government:

US Health Expenditures, Source: National Center for Health Statistics
Paid for, I should add, with your taxes. That means half of our healthcare spending goes through programs of socialized medicine. Whether you like those programs or not, we’re not getting good value for our tax dollars. Single-payer countries spend less per capita on their entire populations:
Canada: $4608 / person
Australia: $4420 / person
United Kingdom: $4003 / person
How is it possible that we spend more on a fraction of our population than they do on their entire population? There are a few classes of reason:
Between the patchwork of programs spending the money and CMS (Medicare, Medicaid, CHIP) being legally barred from negotiating better prices with drug and device manufacturers, we can’t get any of the savings you’d expect from buying in bulk.
Our government programs cover the most expensive people. Sick people are the majority of cost for any insurance program. The US system is just unique in that it segregates ‘cheap’ healthy people into the private sector.
Because we have hundreds of state/local governments and charity care programs (listed under ‘Other Private’ and ‘Other Public’ above), we have not one but hundreds of ‘health systems’ in the US. Systems which duplicate their sophisticated administrative bureaucracies many times over on both the payer and provider sides.
We’re no longer debating whether we should have government-run healthcare. Now we’re just haggling over who gets a slice of the pie.

Healthcare Spending by Age Group in Billions. Source: National Center for Health Statistics
IV. Medicare-for-All Is Not Painless
It’s tempting to dream about Single Payer in the US. We just issue everyone a Medicare card and boom! No more medical bankruptcies, no more premiums, no more deductibles — We made it, we’re…Invincible!

No, You’re a Popsicle
I haven’t reviewed the most popular actual Medicare-for-All plan from Congressman John Conyers Jr., but let’s consider a few of the issues with a hypothetical ‘naive’ conversion.
The private half of US Healthcare puts $1T+ annually in the pockets of providers (hospitals, doctors, etc.) at higher rates than Medicare. What happens when we cut those revenues by 20%?
687,000 people are employed by private health insurers or for billing private health insurers. What should we do about the unemployed?
And there’s pricing: Medicare reimbursement statutorily references private market prices for drugs, medical devices, facility usage, etc. What happens when there’s no private market anymore?
Finally, Medicare isn’t actually a ready-made single-payer program. It has holes and gaps in its coverage. A poorly orchestrated transition to Medicare-for-All could look a lot like the Great Recession in terms of economic impact.
I’d like to review Rep. Conyers’ bill in detail and I have some ideas of my own for a smooth transition, but that would be a post and a half all by itself. You might even say: I have discovered a truly marvelous proof…which this margin is too narrow to contain.

Let’s Wrap It Up
Healthcare is an industry that requires deep knowledge. You are likely familiar with how much training clinicians receive. Well, I was at a Healthcare Revenue Cycle conference once and a speaker asked (via a show of hands): How many years of experience do you have in our industry?
Half the room had 30+ years
A third of the room had 20–30 years
A sixth of the room had 10–20 years
No one had less than 10 years
If you take nothing else from this post, remember this: American Healthcare is very complex. Attempts to reform it without careful thinking are reckless at best. Resist the temptation to nod sagely when people say easy things that sound pretty good. Investigate their conclusions yourself instead.
Talking is easy — Healthcare is hard.
*12% of cases of murder or manslaughter with a known attacker as detailed in the FBI’s 2014 Uniform Crime Report.
**Health insurance has different cost-of-claims than car insurance: ~75% of private health insurance premium dollars go towards claims, unlike 25% among automotive carriers.